COVID-19 Daily Posts Summary & Microembolism Part II
Daily thoughts & numbers on the COVID-19 pandemic from a M.D. working in the front lines at the Emergency Department in a hospital in Stockholm, Sweden.
I created this site in 2018 with the first post published 24th April 2018. My ambition for this site was, and still is, to be a placeholder for links and thoughts I find interesting related to emergency medicine (inspired by other similar sites such as EMCrit, LITFL, and the Swedish site STAIRS). I want this site to be an open node in space, adding to the rich culture of FOAM (Free Open Access Meducation) that exists online and, if it gets any traction, also being part of the online conversation of best practices in emergency medicine. However after the first post life – as it often does – had me prioritizing other projects in my life.
Until now.
Fast forward about twenty months later and enter the COVID-19 pandemic that has changed everything. When COVID-19 had us preparing for hell at my hospital in Stockholm, I then decided to write daily, I started the first daily post on 25th Mars 2020, with the aim to, again, organize links and resources and write down some of my thoughts on the emergency medicine aspects while trying to track the daily numbers of COVID-19 deaths both locally and globally.
It’s now twenty five days later and the number of deaths have accumulated globally from 16 362 to 146 088 and in Sweden from 42 to 1 511.
A lot has happened in the interim of these twentyfive days.
We have mobilized resources, learned more about the SARS-CoV-2 virus, an we seem to have passed the worst peak for now (?), and there’s been huge economic stimulus invested (trillions and trillions of dollars) trying to keep society and as many patients as possible from sinking.
The pandemic is far from over and it will have major repercussions for years to come.
But these daily posts have now served their purpose for me as the scope and the pathology of the COVID-19 pandemic is clearer than it was twenty five days ago. I will still keep updating CTSOP regularly, but not daily, and not always with COVID-19 specific posts – the original aim remains to keep adding resources, links and thoughts relating to emergency medicine (both in English and Swedish, and sometimes in Swenglish as they say).
Finally a summary of the 25 posts and some final thoughts on the microembolism theory presented at day 18.
25 Day Summary:
- 25th March — Are all Systems Go? – A post on preparations before the storm and the mentality of having situational awareness of your resources by checking and rechecking your systems capacity at every shift.
- 26th March — Predicting the Critical. – A post about temporal changes in laboratory markers from illness onset in patients hospitalized with COVID-19.
- 27th March — Treatment Alternativess. – A brief mentioning of a small study where hydroxychloroquine (Plaquenil) combined with the antibiotic Azithromycin was used to treat COVID-19 patients. During this time the hospitals in Stockholm had started to administer Chloroquine to certain COVID-19 patients, something that is no longer done due the lack of effectiveness and to side-effects such as long QT-time.
- 28th March — Exponential Growth. – A look at visualizing the spread and trends of COVID-19 with help of logarithmic scales.
- 29th March — 7 Clinical Observations. – My observations of COVID-19 symptoms and diagnostics from the daily clinical work at the ER.
- 30th March — Timeline. – An attempt to map out some of the key events of the pandemic.
- 31st March — ARDS. – Looking at the age groups and distribution of patients developing severe ARDS and needing intensive care.
- 1st April — Damage Control. – Discussing the ethics of prioritizing patients in light of extraordinary circumstances when resources might become completely overwhelmed (thankfully it never got as bad as we expected (yet?) in Sweden, thanks in large part due to mobilization of resources, and also – perhaps – social distancing policies).
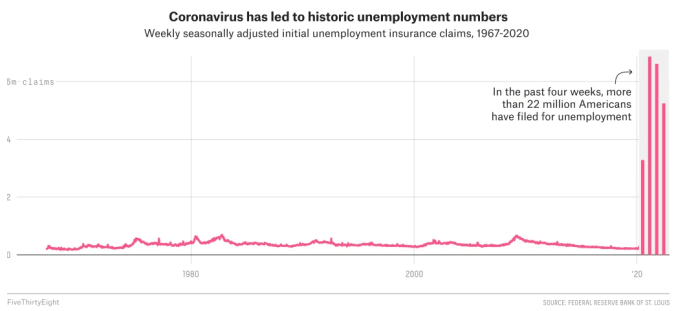
- 2nd April — The Curve. – On death tolls rising around the globe and NY becoming the new urban epicenter of the SARS-CoV-2 virus.
- 3rd April — NOT a Black Swan. – How a virus pandemic was predictable, and how global societies have failed to be prepared despite previous warnings from experts.
- 4th April — Amat Victoria Curam. – Thoughts on the previous theme, but with a focus on Sweden and the last decades extreme political dismantling of the number of critical care beds and hospital beds in general (compared to other developed countries), leaving us with no margins, no buffer, for when shit hits the fan.
- 5th April — Another Night Shift. – A short post due to a crazy week with 6 nights at the hospital, culminating with the worst weekend we have ever seen in our ER.
- 6th April — War-like Scenes in the ER. – As we had our toughest days in the ER with ambulance after ambulance calling in with critically ill patients an article was published at the same time describing similar scenes in the ER of a hospital in NY.
- 7th April — Work Eat Sleep — Repeat. – On the importance of routines in the midst of the storm.
- 8th April — POCUS. – On Point of Care Ultrasound and COVID-19.
- 9th April — STEMI. – Where are all the STEMI patients during this pandemic?
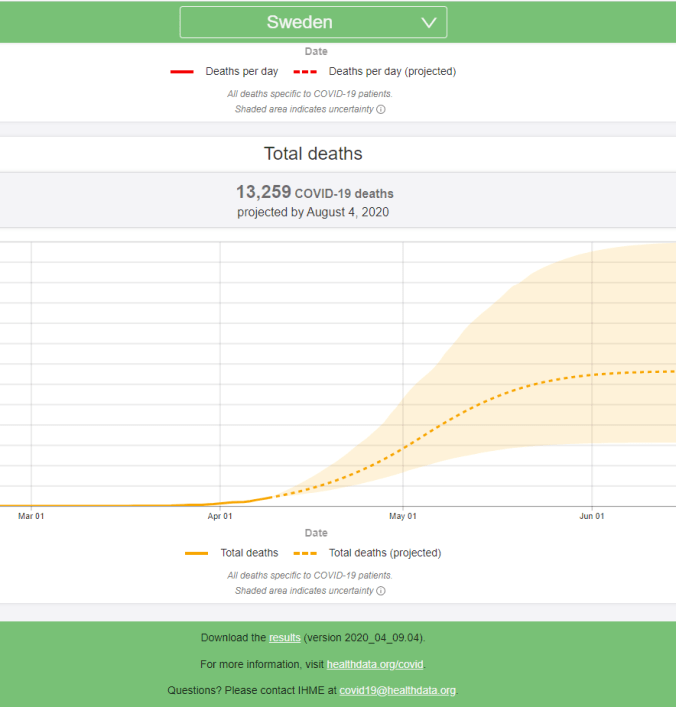
- 10th April — Extubation. – More and more patients getting extubated from our ICU, things are a now a bit calmer again compared to the previous weekend, and one model projection on when we will reach peak pandemic.
- 11th April — Microembolism. – Can Anticoagulants Protect Against Getting Severe/Critical COVID-19 pneumonia/ARDS?
- 12th April — Diarrhea. – The pathophysiology of some patients presenting with diarrhea as a symptom.
- 13th April — CT Features. – A retrospective analysis of 120 consecutive patients from Wuhan city and what the typical CT thorax findings are in these patients.
- 14th April — Phase 2. – Is the worst when it comes to hospital influx and the number of critically ill patients needing intensive care at the same time, behind us in Stockholm/Sweden?
- 15th April — Phenotype L & H. – Categorizing COVID-19 in two types, and how type L is different from severe ARDS (those with type H) , and that there is different optimal treatments for each.
- 16th April — Covid 19 Cytokine Storm. – J Infect 2020-04-10 article by Yeet et al, ‘Cytokine Storm in COVID-19 and Treatment‘.
- 17th April — Aftermath. This pandemic will have lasting effects on society for years to come.
- 18th April. Microembolism part II, summary of the last 25 posts and the last daily post on this pandemic.
Microembolism & Anticoagulants part II
Finally, some additional thoughts on the microembolism theory presented at day 18. In brief: we have seen a considerable decrease of patients with atrial fibrillation in our wards, maybe due to the fact that they are already on anticoagulants that protects them from severe COVID-19 pneumonia, the SARS-CoV-2 virus probably causes (besides lung-embolisms) microembolism in the most critical patients resulting in severe ARDS?
The following report on the cardiopulmonary findings of four autopsies performed on patients within the United States, address thrombotic microangiopathy as a significant finding.
Sharon et al published the report in BMJ 2020-04-06, ‘Pulmonary and Cardiac Pathology in Covid-19: The First Autopsy Series from New Orleans’: *
The dominant process in all cases was consistent with diffuse alveolar damage, with a mild to moderate mononuclear response consisting of notable CD4+ aggregates around thrombosed small vessels, and significant associated hemorrhage. Important additional mechanisms that may have contributed to death in this initial series of autopsies include a thrombotic microangiopathy that was restricted to the lungs. This process may involve activation of megakaryocytes, possibly those native to the lung, with platelet aggregation and platelet-rich clot formation, in addition to fibrin deposition. Small vessel thrombus formation in the lung periphery was in many cases associated with foci of alveolar hemorrhage. In one case, extensive fibrin and early organization was present, with degenerated neutrophils within the alveoli possibly representing neutrophil extracellular traps.
COVID-19 Numbers Sweden 2020-04-18 *
- 1 511 deaths nationally
- 897 of them in Stockholm
- 13 822 confirmed cases nationally
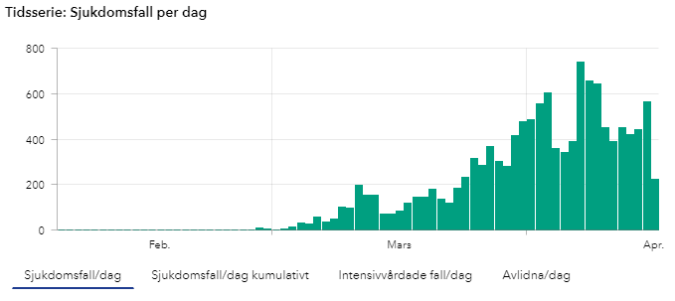
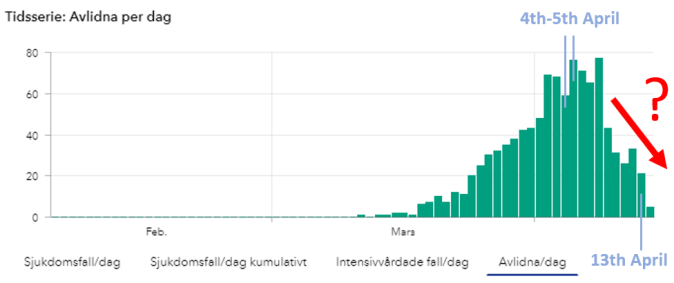
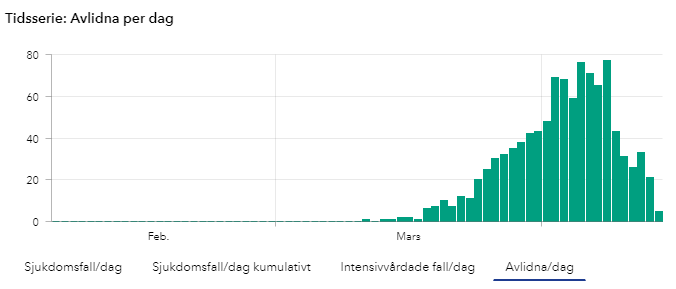
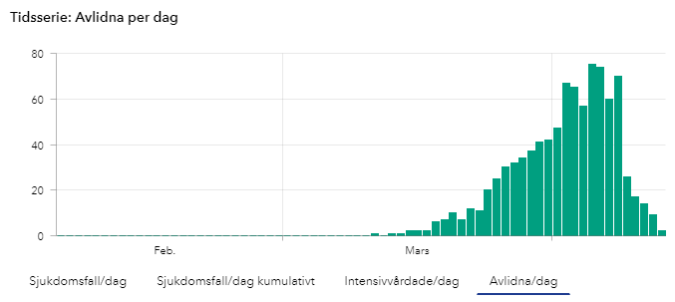
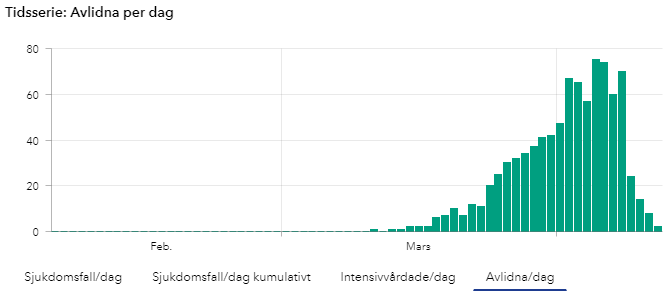
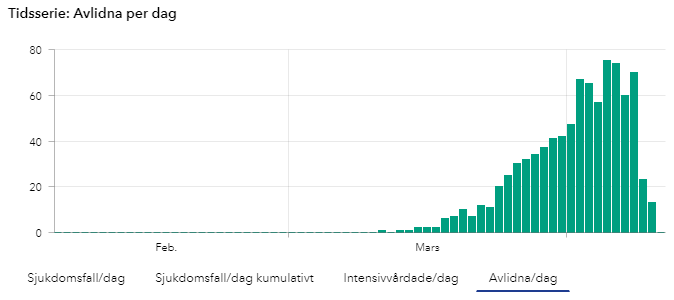
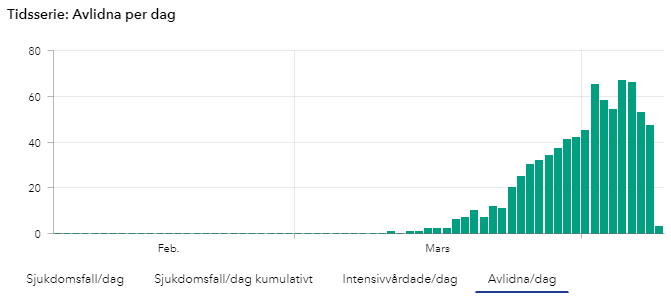
DEATHS [SWE]

New confirmed deaths daily in Sweden.
(Number of COVID-19 cases over time in Sweden, updates during mornings at 14:00 so todays numbers are not yet complete until the next day).
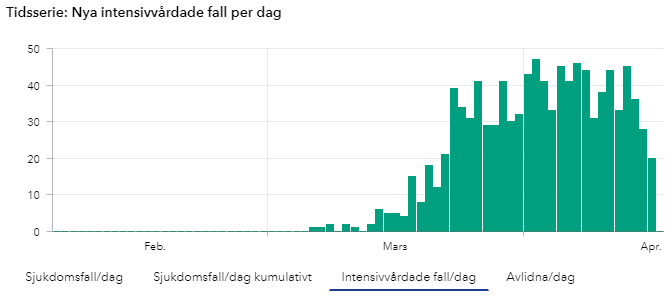
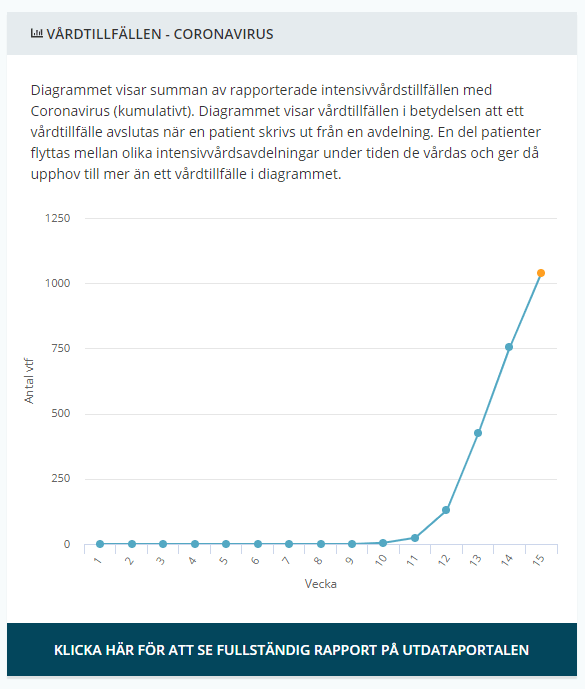
ICU [SWE]

New Covid-19 patients Being Treated at the ICU in Sweden.
(Number of COVID-19 cases over time in Sweden, updates during mornings at 14:00 so todays numbers are not yet complete until the next day).
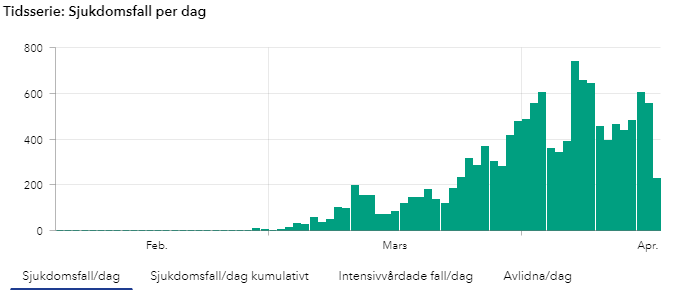
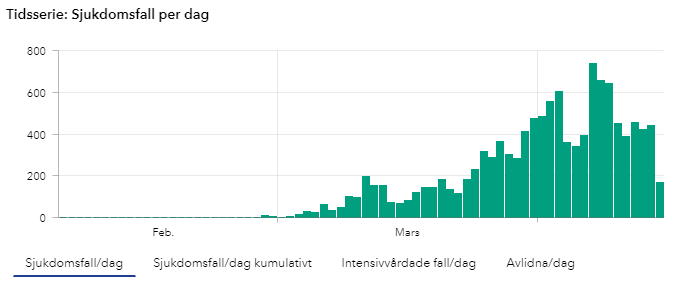
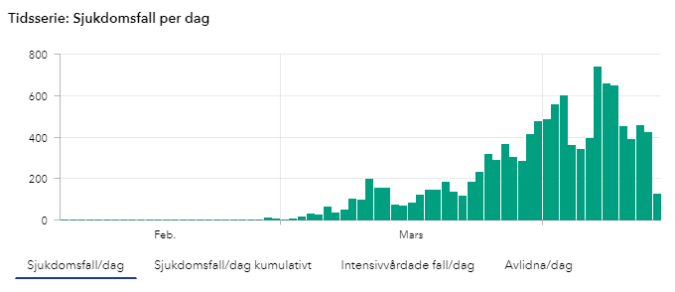
NEW CONFIRMED CASES [SWE]
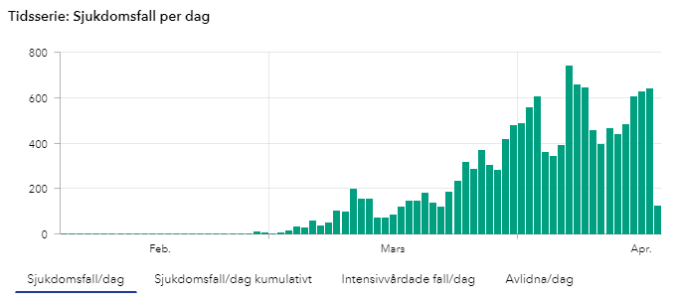
New confirmed cases daily in Sweden.
(Number of COVID-19 cases over time in Sweden, updates during mornings at 14:00 so todays numbers are not yet complete until the next day).
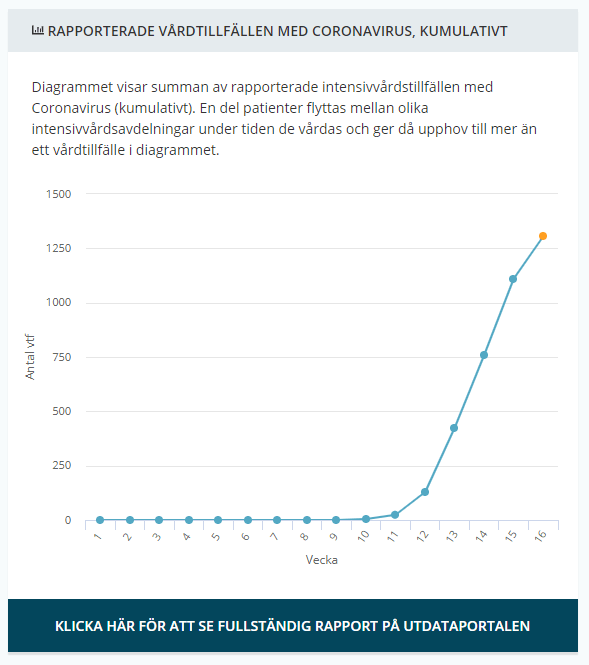
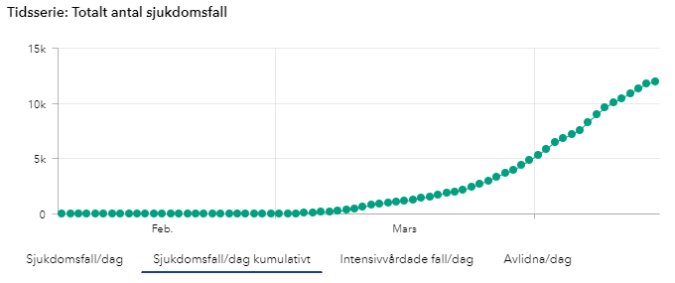
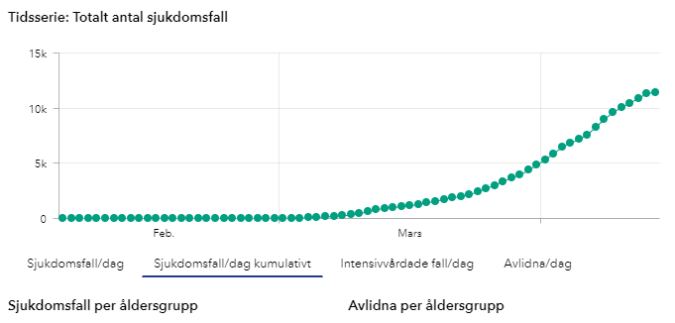
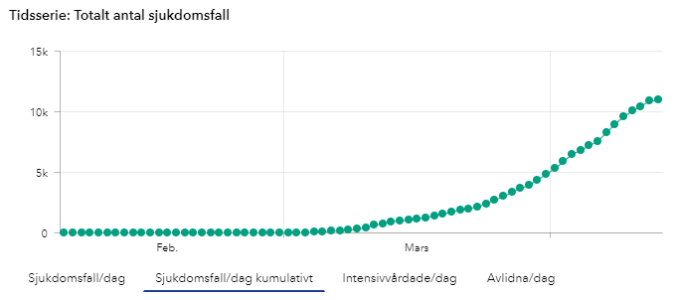
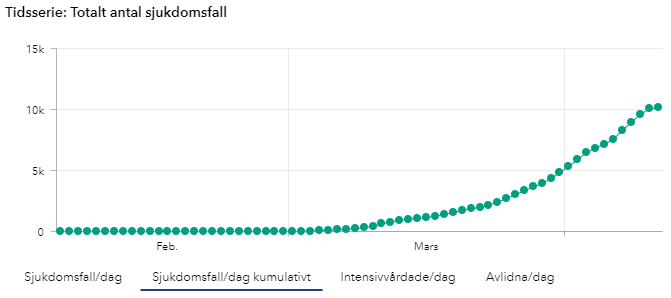
TOTAL CONFIRMED CASES [SWE]
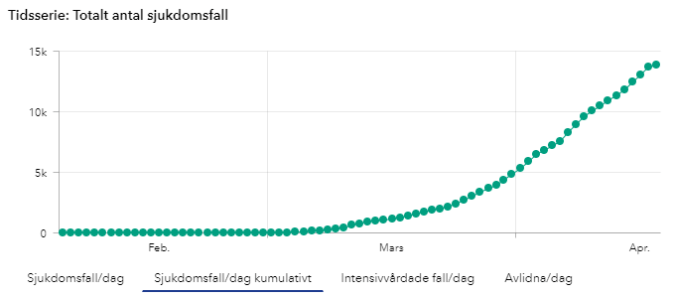
New confirmed cases accumulated over time in Sweden.
(Number of COVID-19 cases over time in Sweden, updates during mornings at 14:00 so todays numbers are not yet complete until the next day).
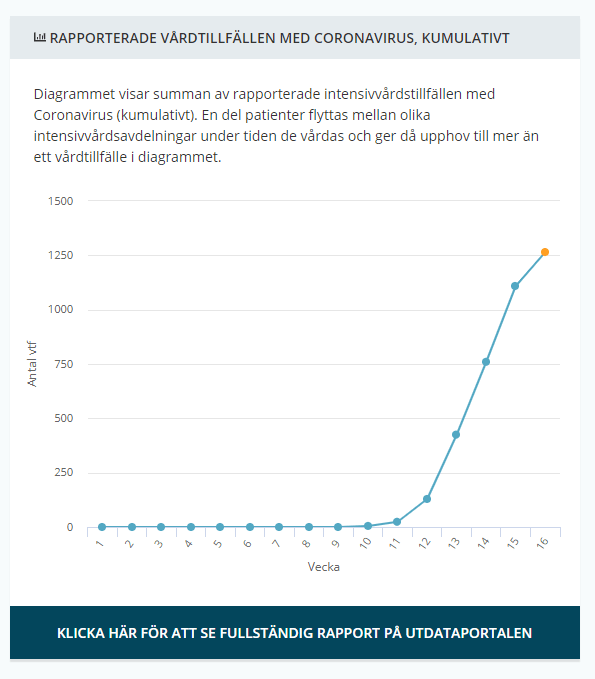
- Intensive care Sweden: *
- 1 042 COVID-19 confirmed patients treated in the ICU in total so far
- 10,6 days from symptoms to ICU
- 25,5 % women
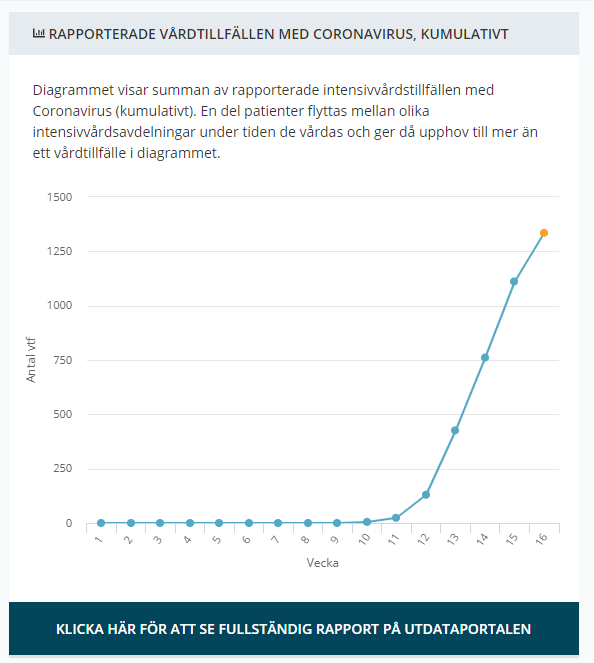
Total number of recorded of COVID-19 patients needing ICU care each week. From Week 10 it seems to more than triple each week for the first 4 weeks. From week ten: 5 → 24 → 129 → 426 → 761 → 1 111 (1 335 this week up until now, however since it’s only saturday this weeks numbers are yet incomplete)
COVID-19 Numbers Globally (updated today 2020-04-18 at 18:00 CET) *
- 146 088 confirmed deaths
- 2 160 207 confirmed cases
- 8 478 new deaths
That’s it for now, this is the last of the daily posts, CTSOP will still update, but not daily, and the theme will be emergency medicine in general and not just COVID-19 specific.
As always, stay calm and keep safe!